
As California faces a growing budget deficit, state lawmakers quietly moved forward with a last-minute budget hearing on April 6 that could direct millions in taxpayer dollars toward sex-rejecting procedures and pharmaceutical interventions for minors.
The hearing, titled “Access to Gender Affirming Care in California,” brought together state agencies, providers, and select panelists to discuss expanding access to what the state broadly defines as “gender-affirming care.”
According to the state’s own materials, this care includes mental health services, counseling, social support, hormone therapy, pharmaceuticals, and in some cases surgical interventions for gender-confused youth.
The document goes on to attack the Trump Administration over its efforts to rein in these interventions, describing the administration’s actions as a systematic effort to “erase transgender people from existence.” It criticizes the Kennedy Declaration by Health and Human Services Secretary Robert F. Kennedy Jr., which declared that “gender-affirming” care for minors is “neither safe nor effective,” and two proposed U.S. Centers for Medicare & Medicaid Services rules that would restrict such care in Medicare/Medicaid-participating hospitals and prohibit federal Medicaid funding for it for youth.
While much of the public conversation focuses on medical treatments, the model being advanced in California goes far beyond clinical care. It is a full-system approach that increasingly runs through public schools.
Programs that are a part of what the state calls “The Master Plan,” such as California’s Children and Youth Behavioral Health Initiative, are already prioritizing early intervention by embedding services directly into school settings. That means gender-related counseling can now take place through school psychologists, wellness centers, and Medi-Cal-funded support services operating on campus.
The result is a system where schools are no longer just centers for education. They are becoming access points for mental health screening, identity-based counseling, and referrals into the broader medical system.
Critics argue this effectively transforms schools into one-stop, one-way ideological hubs, raising serious questions about parental awareness and oversight.
All of this comes as California lawmakers consider an additional $26 million in funding tied to expanding access and delivery of these services.
That new push builds on existing spending. The state has already allocated up to $15 million to sustain gender-related coverage in Covered California plans, while Medi-Cal continues to cover related treatments, including mental health services and pharmaceuticals.
During the hearing, California State Senator Caroline Menjivar, who co-chairs the committee, opened the hearing by claiming, “The Trump Administration has meticulously and inhumanely attacked the LGBTQ community, specifically the trans community.”
Tyler Sadwith, the Chief Deputy Director of Health Care Programs and State Medicaid Director of the Department of Health Care Services, testified that sex-rejecting procedures are effective, medically necessary, and that they improve health outcomes.
Assemblyman Joe Patterson, however, urged his fellow committee members to look at the scientific evidence showing that “gender-affirming” surgeries are harmful.
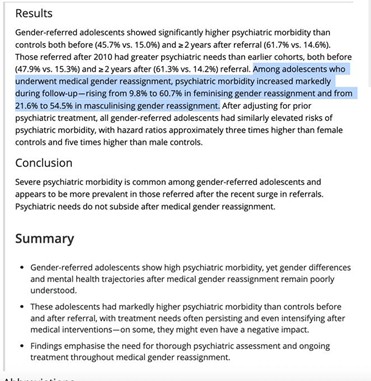
Patterson is right. A new Finnish study reports that youth gender transitions for patients under age 23 did not improve mental health symptoms. For some youth, medical gender reassignment may have even had a negative impact, according to the research.
So why the urgency to expand funding now, especially in the middle of a deficit? The panelists and committee members in support repeatedly blamed federal actions by the Trump administration, which have not only cut off funding but also informed hospitals they will lose Medicare if they continue to offer treatments to minors deemed not safe and not effective.
The structure of the hearing itself is also raising eyebrows. The official agenda shows a lineup dominated by state agencies, advocacy organizations, and selected providers and patients who support the medical transitioning of minors. Dissenting medical voices and parents’ rights groups were notably absent. It’s not difficult to figure out why.

Among those featured was Dr. Johanna Olson-Kennedy, a prominent figure in pediatric gender medicine. Johanna Olson-Kennedy, who played a key role in pushing youth gender care in the recent California budget hearing, has become a lightning rod for controversy. She led a taxpayer-funded NIH study on puberty blockers but delayed publishing results that reportedly showed no clear mental health benefit, raising serious concerns about transparency. She is also being sued by a detransitioned former patient who alleges she rushed diagnosis and treatment without adequate safeguards. Critics argue her approach minimizes psychological screening for minors, while her involvement in policy and legal battles has blurred the line between physician and activist.
The lone dissenter on the committee questioning puberty blockers, cross-sex hormones, and surgeries for children at the taxpayers’ expense was Joe Patterson, a Republican California Assemblyman. He asked Dr. Johanna Olson-Kennedy if she supported medical interventions for children without parental consent. The doctor emphatically stated she would not support that, citing the reason that transitioning a child without a supportive parent does not work.
One of the presenters, identified as Jane Doe, shared her experience as the parent of a child born female who now identifies as male. She said her child first expressed identifying as a boy at age 5, and by age 8, the family supported a name change and social transition at school. Doe described herself and her husband as Air Force veterans and “progressive feminists,” and said they have consistently affirmed their child’s transition. She testified that at age 11, their child underwent a medical procedure to receive a puberty blocker implant. According to Doe, changes under the Trump Administration have led TriCare to deny coverage, leaving the family with approximately $200,000 in medical costs—which illuminates the astronomical costs of medically transitioning children at the taxpayers’ expense.
This was not a balanced debate. It was a coordinated presentation. There were no medical experts allowed to present studies that show that these interventions do not improve mental health or the irreversible lifelong side effects.
Public comment was included, but the timing of the hearing, announced just before a major holiday weekend, limited broader participation.
Moreover, public comment was scheduled for the end of hearing, and the public was only allowed to comment for 30 seconds each. This included Erin Friday, a parent who was reported to Child Protective Services by Dr. Johanna Olson-Kennedy, as well as detransitioner Layla Jane, who was prescribed puberty blockers and testosterone at age 12 and a double mastectomy at age 13.
California Democrat Caroline Menjivar, co-chair of the committee, who supports using taxpayer money to medically transition innocent children, refused to address concerns raised by these parents and detransitioners. Instead, she smiled at them, saying they should only speak about mass shootings, while she herself speaks on a wide range of issues.
Governor Gavin Newsom has made clear that California intends to lead the nation on expanding access to gender-related care, particularly for minors. In a recent podcast with the New York Times, Newsom told Ezra Klein, “I want to see trans kids… I have a trans godson. There’s no governor who has signed more pro-trans legislation than I have.” The April 6 hearing reflects that priority. It was not framed around whether these services should expand, but how quickly and how far.
What is happening in California is not just a policy change. It is a structural shift. Schools are becoming entry points into medical systems. Mental health services are increasingly tied to identity frameworks. State funding continues to expand even as financial pressures mount, and without sufficient transparency, debate, or even acknowledgment of the long-term evidence that shows sex-rejecting interventions result in long-term irreversible harm, including infertility.
At a time when California is facing serious fiscal challenges, lawmakers are advancing policies that reshape both healthcare and education at the same time. The real question is whether the public fully understands what is being built before it goes even further.